Patient Recruitment 80% of trials miss their enrollment deadline. Almost none of it is the drug's fault. Most enrollment post-mortems look at the protocol, the therapeutic area, the competition for patients. They rarely look at the ninety seconds a frightened person spent on a phone at 11pm, deciding whether your site was real. Around eight …

Patient Recruitment
80% of trials miss their enrollment deadline. Almost none of it is the drug’s fault.
Most enrollment post-mortems look at the protocol, the therapeutic area, the competition for patients. They rarely look at the ninety seconds a frightened person spent on a phone at 11pm, deciding whether your site was real.
Around eight in ten trials run behind their original enrollment timeline. The science is usually not the reason. The reason is friction, spread across every point where a nervous human has to take one more step toward you, and quietly decides not to.
Most patient recruitment advice is written for sponsors buying a recruitment vendor. This one is written for the research site itself, and for the part of recruitment the site actually controls. Twelve truths, short and unfiltered. Little of it is complicated. Most of it is ignored.
How fast should a site respond to a patient inquiry?
Within the hour. A patient rarely inquires with one site. They fill in a form, keep scrolling, and fill in two more. The site that answers first is usually the site that enrolls them, and the window is measured in minutes, not days.
- Speed beats everything.Call a new inquiry within the hour, or another site calls first.
- Make referring a thirty-second act.If a physician needs a fax to send you a patient, the referral is already gone.
- Use AI to triage, never to talk.Automate the matching. Never automate the first human call.
The window is short and it does not reopen. Everything downstream in your enrollment number depends on being the site that moved while the patient was still deciding.
Does a website affect clinical trial patient recruitment?
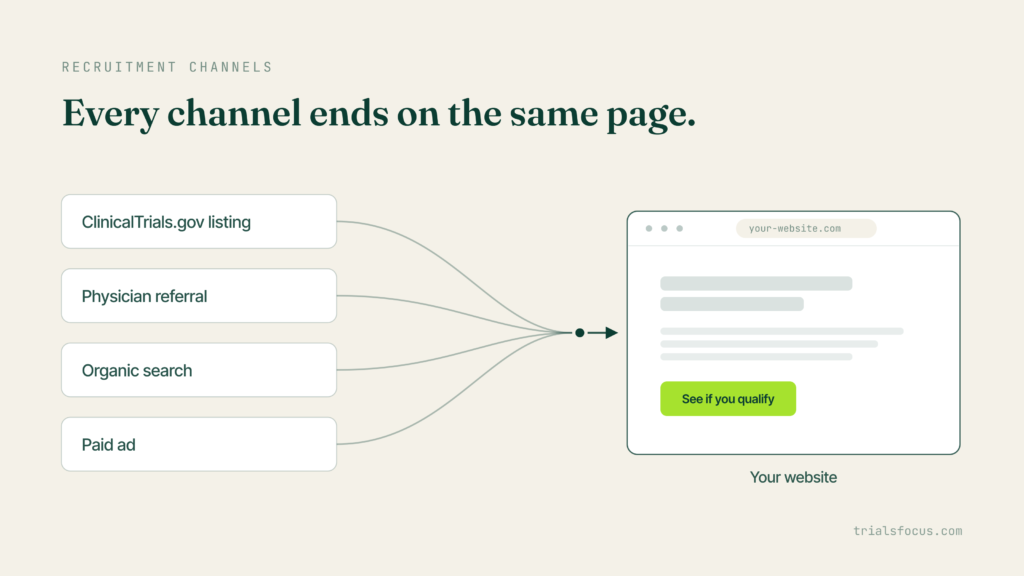
Yes, and more than most sites account for. Almost every recruitment channel ends in the same place: a listing on clinicaltrials.gov, a physician referral, an organic search, a paid ad. Different starting points, one destination. For most patients, the website is where they meet the site before anyone speaks to them, and it is doing the talking whether or not it was built to.
- One study, one page.A dedicated landing page out-enrolls a homepage every time, because it answers one question instead of forcing a choice.
- Write for a scared human, not a regulator.Sixth-grade reading level, or they leave before they reach the part that matters.
- Mobile or invisible.They find you at 11pm on a phone. Be fast there, or be nowhere.
- Kill the stock photos.Real faces, a real principal investigator, a real address. Generic reads as fake to someone who is already unsure.
None of this is about polish. Each item removes one reason a nervous person had to hesitate, and hesitation is where patients are lost.
Why do eligible patients not enroll?
Because trust fails before eligibility is ever tested. This is the order most sites get backward, and it quietly costs them patients who would have qualified.
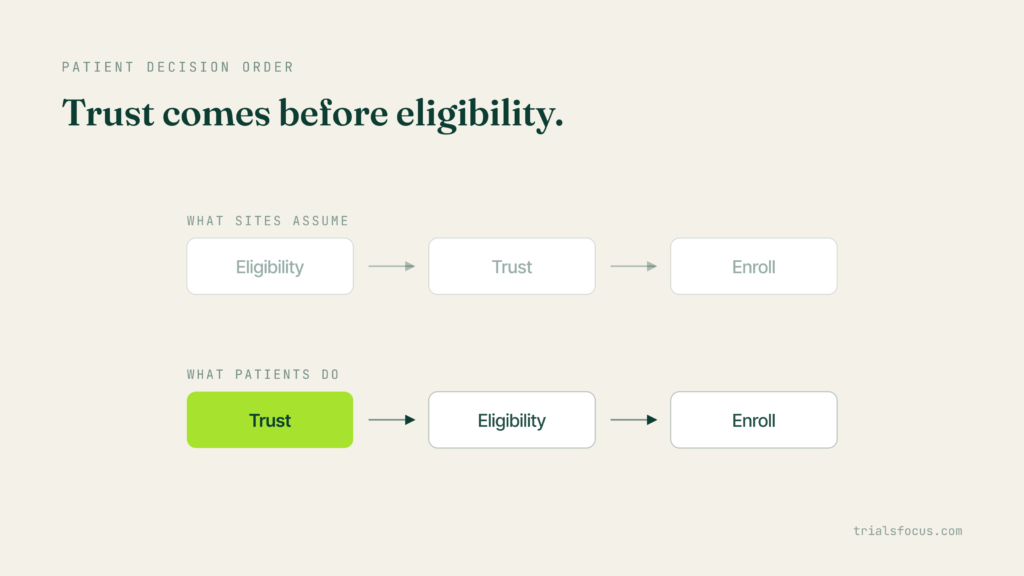
- Trust before eligibility.Patients decide you are real before they check whether they qualify. If the trust is not there, they never reach the eligibility question, and the site never learns they existed.
- Diversity is design now, not outreach.Recruit where the disease lives, not where outreach is easy, and yes, regulators are watching.
- Community out-converts ads.Patients trust advocates and peers long before they trust your campaign, so show up where that trust already lives.
Build the trust first, and eligibility becomes a conversation the patient wants to have. Skip it, and the most eligible patient in your area still leaves.
What should a site measure in patient recruitment?
Randomized patients, not leads. The metric a site watches shapes the behavior it rewards. Leads are easy to count and easy to feel good about. They are also where budgets quietly disappear.
- Stop counting leads. Count randomized patients.The gap between the two is where budgets die, and it is usually invisible until the study is already behind.
- Retention is recruitment.A dropout costs more than a no-show. Budget to keep patients, not just to find them.
A site that tracks inquiries looks busy right up until the enrollment report arrives. A site that tracks randomizations finds the leak while there is still time to fix it.
Why do clinical trials miss their enrollment targets?
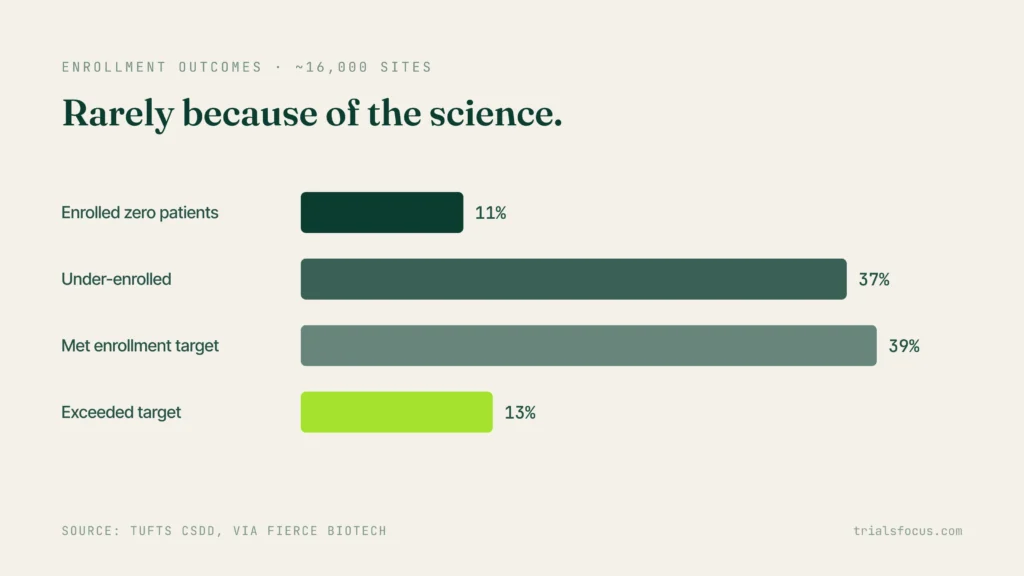
Rarely because of the science. Around eight in ten trials run behind their original enrollment timeline, and the cause is almost always operational and human: the patients existed, and the path to enrollment asked more of them than they were willing to give.
The site-level data shows how uneven this is. Across roughly 16,000 sites, Tufts CSDD found that about 11% enrolled no patients at all and 37% came in under target, while 39% met their number and 13% exceeded it.
Read that as a distribution, not an average. Sites running comparable protocols in comparable therapeutic areas land in completely different places. Very little of that spread is explained by the drug. Most of it is explained by the twelve frictions above, each one small enough to ignore and cheap enough to fix.
The person behind the number
None of this is about a fancier website. It is about remembering there is a frightened person behind every number on the enrollment chart, and building each step so it is easier for them to take.
That is the part we care about at Trialsfocus. Not a homepage that looks impressive to the people who already work at the site, but the page a scared patient actually lands on at night, and whether it makes the next step feel safe and obvious. If your enrollment is coming in behind and you suspect the patient side of your website is part of it, we are glad to open it with you and read it the way that patient would.
For the other half of the picture, the moment a sponsor evaluates your site before you ever speak, see What a CRO Site Selector Sees in the First 60 Seconds.